 PHOENIX, Ariz. — Headache disorders are among the most common health problems worldwide and one of the most underdiagnosed and undertreated, according to the World Health Organization (WHO). In this expert alert, neurologist Amaal Starling, M.D., a headache and migraine expert at Mayo Clinic in Phoenix, offers tips to prevent and manage headache disorders, including migraine and medication-induced rebound headache. There are more than a dozen different types of headache disorders. The most common disabling headache disorder is migraine. It affects more than 1 billion people around the globe, including 1 in 5 women, 1 in 11 children and 1 in 16 men, and according to WHO, is one of the world’s most disabling diseases, Dr. Starling says. Migraine disease can differ depending on a person’s stage in life, she says. “Infant colic is thought to be the infant variant of migraine. Abdominal migraine and cyclic vomiting syndrome are migraine variants that are common in children,” Dr. Starling says. “More classic migraine attacks occur throughout adulthood. In the older adult, the pain associated with migraine lessens; however the associated features such as light sensitivity, sound sensitivity, nausea, vomiting, or aura may be more prominent.” Despite advances in treatment and prevention options, migraine remains underdiagnosed and therefore undertreated, Dr. Starling says. If someone has head pain that makes it difficult to function, odds are that it is migraine; often people think they have sinus headache when it is really migraine. Migraine is a primary headache disorder, meaning it is caused by abnormal function in the brain. Unlike secondary headache disorders, it may not be a symptom of an underlying illness such as an infection or a tumor. Other common primary headache disorders include cluster headache, which occurs in bouts of attacks lasting from weeks to months and typically includes intense pain lasting up to three hours in or around one eye; and tension headache, which usually comes with mild to moderate pain and can be chronic. Some primary headache disorders are associated with certain activities, such as cough headache, sex headache and exercise headache. They also can be triggered by drinking alcohol, eating certain foods such as processed meats containing nitrates, lack of sleep, poor posture, stress and missed meals. “Migraine triggers are very individualized. A trigger for one patient may not be a trigger for the next patient,” Dr. Starling says. “In general, I recommend eating an anti-inflammatory Mediterranean-style diet with fruits, veggies, nuts, legumes; eating foods high in magnesium, eating whole foods, and avoiding processed foods and fasting,” she says. “More recently there has been some data that recommend consuming more omega-3 fatty acids by eating fatty fish such as salmon, sardines, and mackerel.” Overuse of pain medication, including taking nonprescription analgesics such as aspirin and acetaminophen or prescription medications such as opioids and some migraine medications more than twice a week, can trigger rebound headache, also known as medication overuse headache. “If someone is having migraine attacks four or more times a month, it is time to consider preventive treatment,” Dr. Starling says. “If someone has infrequent migraine attacks, occurring less than four times per month, a migraine-specific treatment as needed may be more effective than over-the-counter analgesic medications such as ibuprofen.” New treatments for migraine include the discovery of a new family of preventive medications that target one of the body’s systems believed to be a culprit, the calcitonin gene-related peptide system, and the development of medical devices to treat migraine, she says. If patients have head pain that is reducing their ability to function, rather than diagnosing themselves and self-medicating, it is best to see a health care provider for help managing symptoms, Dr. Starling says. “Over the past several years there has been an explosion of treatment options for migraine attacks and migraine prevention,” she adds. “We have many treatment options to improve the lives of those living with migraine.” Sharon Theimer Mayo Clinic Public Affairs, PREVIOUS ARTICLES:

0 Comments
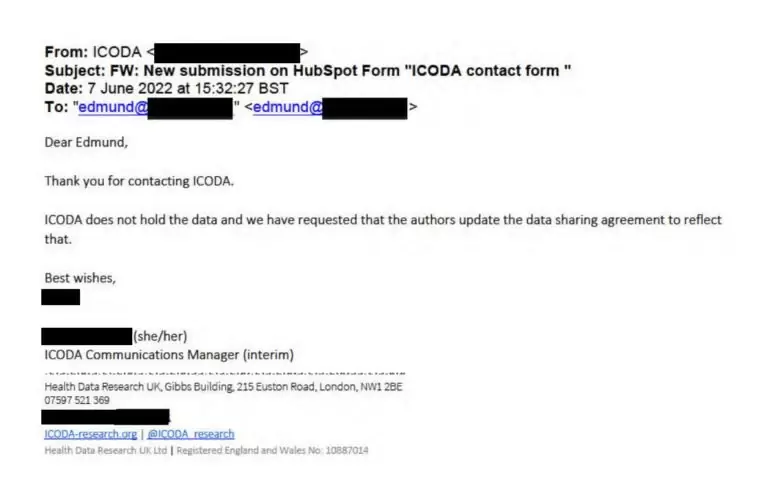
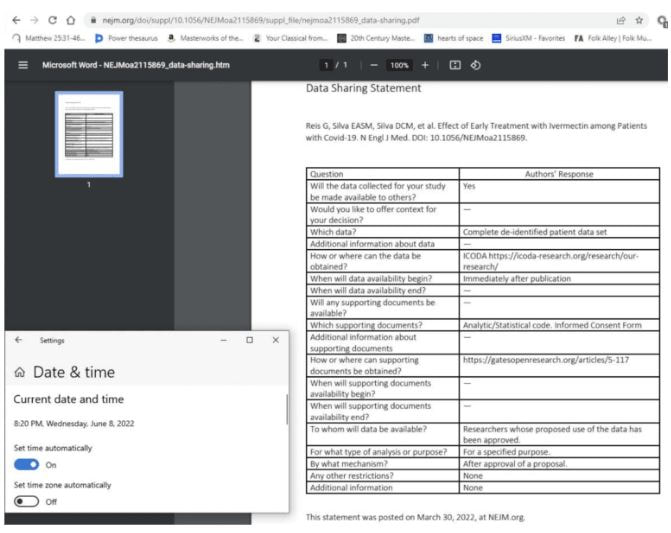
-World Council for Health Following the release of the TOGETHER Trial results to the press in August 2021, media headlines quoted that ivermectin had ’no effect whatsoever’ when used for Covid-19. This press release from TOGETHER Trial investigators influenced international health policy to withhold ivermectin for the prevention and treatment of Covid-19 despite compelling evidence from numerous independent experts, scientific papers, and real world data that mass administration of ivermectin would be effective and safe for Covid-19. The final report of the TOGETHER Trial, published in March 2022 in the New England Journal of Medicine, has major discrepancies in the data compared with what was published by the media more than six months earlier in addition to serious methodological inconsistencies that must be brought to light. Despite numerous requests by international scientists to address these issues, none has been forthcoming by TOGETHER Trial authors. Probable Scientific Misconduct UncoveredA breaking development has highlighted the probability of scientific misconduct associated with this trial, when the manager of the International COVID-19 Data Alliance (ICODA) confirmed that its website, to which the TOGETHER trial has been directing inquiries for deidentified patient data since the study’s publication on March 30, never actually hosted the study’s data. Dr. David Scheim, Dr. Edmund Fordham, and Professor Colleen Aldous have sent a letter (part of which is included below) to the TOGETHER Trial authors, the NEJM Editor-in-Chief, and others asking for the data to be made available immediately or to retract the paper. Call for ActionThis is not the first time that attempts have been made to manipulate data and scientific manuscripts to undermine the evidence that shows ivermectin is effective against Covid-19. The World Council for Health urges journalists, scientists, and civil society to focus due attention on TOGETHER Trial investigators so that they reveal what has been hidden. The World Council for Health supports the use of ivermectin for the prevention and treatment of acute Covid-19, Long Covid, and for Covid-19 vaccine injury under the supervision of trusted health practitioners. BREAKING: The TOGETHER trial data was never at its cited ICODA repository or otherwise availableDear coauthors of Reis et al., 2022,1 the Editor-in-Chief of the New England Journal of Medicine; and (cc’d) editors of other scientific journals, science reporters, bioethicists and other distinguished scientists: In a breaking development yesterday, we learned that the TOGETHER trial has misdirected inquiries to a web repository that never hosted its data, thereby denying the scientific community access to the underlying data for its ivermectin arm since that study’s publication on March 30. A manager of the ICODA data repository emailed us yesterday that its website, to which the TOGETHER trial has been directing inquiries for deidentified patient data since the study’s publication on March 30, never hosted the study’s data.
This took two months to ascertain, in part because ICODA’s listed telephone number still gives the recorded message, “you have reached a number that is not currently set up to receive calls.” Given this flagrant breach of scientific ethics in thwarting access to data with a spurious link, the four outcome measures that scientists have repeatedly requested since April 11, comparative per protocol death and hospitalization rates, treatment vs. placebo, should be disclosed immediately. Note that these are the key outcomes of interest, since both the NIH and FDA found the study’s nonstandard primary outcome measure to be inadequate. It is especially troubling that study co-author Dr. David Boulware evaded our May 10 request for the study’s four key outcome numbers (email thread below) by misdirecting, once again, to this spurious link to ICODA, which never hosted the TOGETHER trial’s data.  The degree of data irregularities and concealment of data here is of a scale unmatched since the Surgisphere scandal of June 2020, which resulted in retractions in the New England Journal of Medicine (NEJM, the publisher of this March 30 study) and in the Lancet. As noted, the study coauthor cited above who replied twice in response to our May 10 letter could not furnish even the simplest accurate information about the study data, its repository location. It is therefore imperative that a study coauthor who can accurately report on this data immediately disclose to the scientific community the four numbers for comparative per protocol death and hospitalization rates as repeatedly requested since April 11. Expedited access to “complete deidentified patient data,” as the study promised beginning “immediately after publication,” on March 30, must also be provided. If these are not provided promptly, we request that the NEJM retract this study. Sincerely yours, David E. Scheim, PhD, US Public Health Service, Commissioned Corps, Inactive Reserve, Blacksburg, Virginia, USA Colleen Aldous, PhD, MASSAf (fellow, Academy of Science, South Africa), School of Clinical Medicine, College of Health Sciences, University of KwaZulu-Natal, Durban, South Africa Edmund J. Fordham, PhD (Cantab) FInstP, EbMCsquared CiC, Bath, England 
Digital Medical Certificate, AltHash Health Blockchain
With the Pandemic much falsified medical certificate has been spreading. The blockchain-based database provides authenticity, immutability, and security of Data. Hence, it is but logical that medical certificates be stored in the blockchain. It also maintains Data Privacy. Last 2018-19 we introduced this project to the Philippines.
What is the main purpose of blockchain?
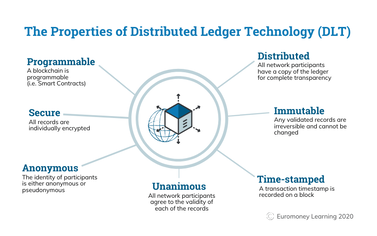
The goal of blockchain is to allow digital information to be recorded and distributed, but not edited. In this way, a blockchain is the foundation for immutable ledgers, or records of transactions that cannot be altered, deleted, or destroyed.
Blockchain is an emerging technology being applied for creating innovative solutions in various sectors, including healthcare. A Blockchain network is used in the healthcare system to preserve and exchange patient data through hospitals, diagnostic laboratories, pharmacy firms, and physicians.
Is there a healthcare blockchain?
At this time, the most common use cases of blockchain in healthcare leverage smart contracts capabilities for medical supply chain, health-credential and vaccination validation, provider credentialing, patient data security, and life sciences clinical study-related data.
The problem in Medical Certificate Issuance experienced in the Philippines One of the challenges in the issuance of medical certificates is the falsification of the document. Doctors most of the time receive inquiries and complaints from health insurance companies or the human resource departments on the certificates submitted by the sick employee. Often times the company doctor or nurse be it from HR/School? or insurance would have to confirm or call the issuing physician on the diagnosis, medication, or recommendation written in the medical document. This oftentimes causes doubt about the credibility of the Doctor. Worst case scenario is when a crime is committed by manufacturing fake medical certificates using an innocent doctor's name and his medical license. This recently happened in Quezon City. 
An article by CNN about the problem
""Police raid print shop producing fake medical certificates of COVID-19 results( Metro Manila (CNN Philippines, July 23) Police on Thursday raided a printing shop in Quezon City for allegedly producing fake medical certificates of COVID-19 results. The Quezon City Criminal Investigation and Detection Group (CIDG) organized an entrapment operation in the afternoon at Brgy. Pasong Putik after a social media post went viral exposing the scheme. Authorities arrested two employees and confiscated the printers, computers, and other hardware as evidence." Full Article. Read More....

IT IS A CRIME
Section 1. Article 174 of Section 5, Chapter 1, Title IV of Act No. 3815 FALSIFICATION OF MEDICAL CERTIFICATES IS A CRIME AND IS PUNISHABLE BY LAW Penalty: The penalties of [arresto mayor] PRISIONCORRECCIONAL in its maximum period to [prision correccional] PRISION MAYOR in its minimum period and a fine not to exceed [1,000] TWO HUNDRED THOUSAND PESOS (P200,OOO.OO) WITH SUBSIDIARY IMPRISONMENT This is where we come in, Digital Medical Certificate
A secure, private and confidential way of creating Medical Certificate by a Medical Doctor. It gives practicing physicians the assurance that their issued certificates, were not corrupted, falsified. Likewise for the Human resource department who receives the medical certificate that the document is true and authentic
Why is Blockchain based Medical Certificate Secure?
Key things: a. Data is cryptographically stored using SHA 256 or Secure Hash Algorthm "SHA-256 stands for Secure Hash Algorithm 256-bit and it's used for cryptographic security. Cryptographic hash algorithms produce irreversible and unique hashes. The larger the number of possible hashes, the smaller the chance that two values will create the same hash. It is developed by NSA" 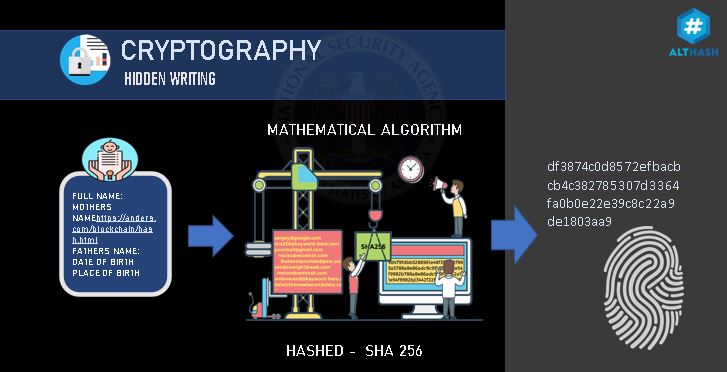
Hashing is the process of scrambling raw information to the extent that it cannot reproduce it back to its original form. It takes a piece of information and passes it through a function that performs mathematical operations on the plaintext. This function is called the hash function, and the output is called the hash value/digest.
b. the cryptographic data can be decrypted using a private and public key Ecnycryption,
" Only the owner of the private key can encrypt data so that the public key decrypts it; meanwhile, anyone can encrypt data with the public key, but only the owner of the private key can decrypt it. Therefore, anyone can send data securely to the private key owner." 
c. The Encrypted Data is stored in a distributed ledger an independent, autonomous node of computers.
For a Criminal to corrupt the Data stored in the MEdical Certificate done by the private physician he has to:
a. decrypt the SHA 256 " As of 2021 technology, the chance of solving a hash with SHA256 algorithm, that is, converting it to the main input, is very very low possibility" b. access the private key of the issuing Doctor " Hackers can infiltrate wallets and steal bitcoins if they know a user's private key." c. hack all the autonomous, anonymous, distributed nodes (all over the globe) which participated in the blockchain network. not including the consensus mechanism of verification on each block. "A blockchain's decentralized nature means that its network is distributed across multiple computers known as nodes. This eliminates a single point of failure. In other words, there is no way to “cut the head off the snake” — because there isn't any head." WATCH DEMO VIDEO ON DAPP (DECENTRALIZED APPLICATION) DIGITAL MEDICAL CERTIFICATE
Blockchain used cases in healthcare to preserve the integrity of the document, and integrity of Physicians and save a lot of money for Companies and insurance paying for fake/falsified documents.
Only a licensed Medical Doctor can have access to and create the Certification. AltHash follows strict background checks to confirm Physicians' application to use the AltHash Health Blockchain

Dr. vincent Rey Vicente, MD is a practicing medical professional, a senior faculty of AltHash University. At present he is also the Business Developement Director of theInternationcouncil of Registered Blockchain Professionals (ICORBP). He introduced Digital Medical Certificate to private medical practices in Davao City, Philippines in addition to the Digital Birth Certificate.
The lining of your digestive tract — like every surface of your body — is covered in microorganisms, mostly bacteria. This microecosystem, called a microbiome, plays a large role in your health. Your mood and behavior also may be impacted by the microorganisms living in your microbiome.
You may be surprised to hear your gut houses up to 1,000 different species of bacteria. By nourishing different types of bacteria, you can keep your microbiome in balance. What you feed your microbiome matters. Most healthy adults can safely incorporate prebiotics and probiotics to their diet. A healthy microbiome promotes a healthy immune system and supports a weight management plan. 
There are two ways to maintain a healthy gut:
In a large bowl, combine the oats and hot water. Let sit for 1 to 2 minutes until the oats are creamy and tender. Stir in oil and sugar; set aside to cool slightly. In a medium bowl, combine the flours, baking powder, baking soda, salt and ground cinnamon. Whisk to blend. Add the milk, yogurt and banana to the oats and stir until well-blended. Beat in the egg. Add the flour mixture to the oat mixture and stir until just moistened. Place a nonstick frying pan or griddle over medium heat. Once hot, spoon ¼ cup pancake batter into the pan. Cook for about 2 minutes, until the top surface of the pancake is covered with bubbles and the edges are lightly browned. Flip the pancake and cook for another 2 to 3 minutes. Repeat with remaining pancake batter.
Nutrition information per two-pancake serving: 192 calories, 6 grams fat, 0 grams saturated fat, 0 grams trans fat, 4 grams monounsaturated fat, 302 milligrams sodium, 30 grams total carbohydrate, 2 grams dietary fiber, 6 grams protein 
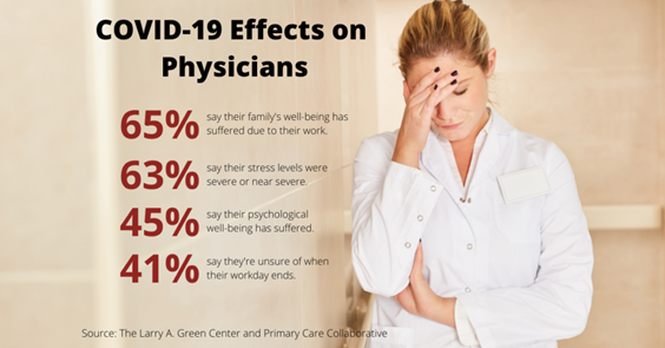
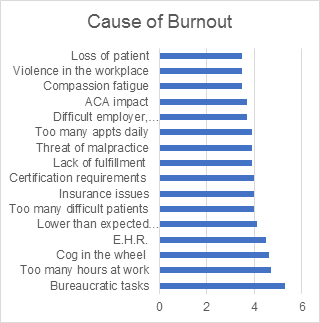
You may also be interested in other articles:When physicians lament they feel burned out at work, what exactly do they mean?  Here's how one doctor describes conditions that lead to burnout: "I barely spend enough time with most patients, just running from one to the next; and then after work, I spend hours documenting, charting, dealing with reports. I feel like an overpaid clerk." Physicians experiencing work burnout don't always find relief at home. "Home is just as busy and chaotic as work. I can never relax," another physician says.  The Medscape Physician Burnout & Depression Report 2022: Stress, Anxiety and Anger report sparked impassioned responses from physicians on several fronts. In that report, 47% of physicians who responded said they were experiencing burnout, up from 42% in our survey from 2021. Few Doubt the Burnout/Depression ProblemWhile opinions differ about the chief culprits, commenters lamented rather than questioned the extent of burnout and depression among physicians. "What is striking to me is, 24% of our colleagues are suffering from clinical depression," one doctor worried. "This is a serious matter. Individuals need to address a work-life balance. Find ways to seek help, and [develop] a coping mechanism."
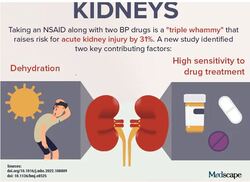
 "I am sympathetic, but medical schools should do a better job in choosing and teaching students that being a doctor requires having a vocation for it. That's not the same as being a do-gooder," one physician argued. "It's having a passion for medicine and practicing it." The Right Employer and Community Help DoctorsHow possible is it to put together the right combination of employer and vibrant community that avoids burnout? That question generated a lively back-and-forth. "Get your degree, do your residency, then say goodbye to corporate medicine and do direct primary care," one doctor advised. "You will pay off your loans and have fun doing it!" Another physician shot back, "Good luck launching an independent practice in a community with amenities that let you lead a full and enjoyable life away from work." Certainly research shows a healthy work-life balance and a rewarding personal life positively affect burnout and depression among physicians. Some believe relaxation is more attainable in self-employment vs corporate employment, but that assumption has not always proved true. The right choice for a doctor's mental health is sometimes elusive and is affected by many factors. 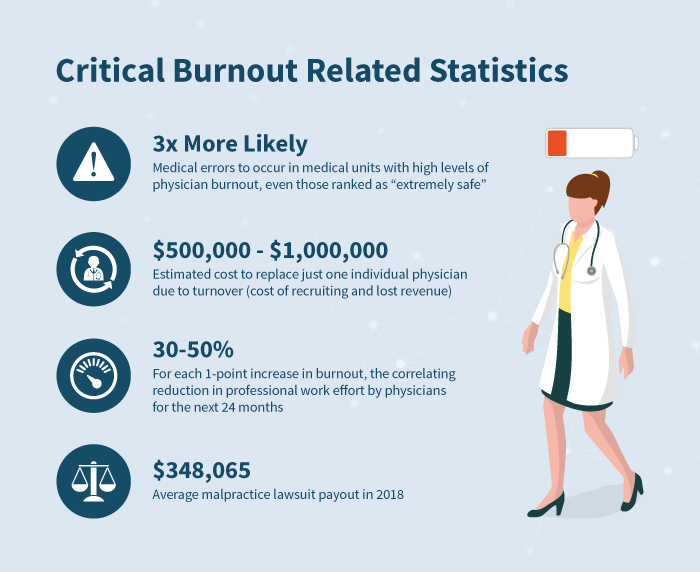 Credits: Images: E+/Getty Images Medscape Medical News © 2022 Cite this: Jon McKenna. Physicians React: Burnout Rates Are Alarming, so Who Should Drive Change? - Medscape - Jun 06, 2022.  A new study investigating a dangerous "triple whammy" in patients taking blood pressure (BP) medications, research into complications from cancer regimens, and recent findings about treatment and prevention concerns resulted in kidneys becoming this week's top trending clinical topic. The combination of three drugs — a diuretic; a renin-angiotensin system inhibitor, such as an angiotensin-converting enzyme (ACE) inhibitor or angiotensin receptor blocker; and a nonsteroidal anti-inflammatory drug (NSAID) — increases the risk for kidney injury. New research has identified the mechanism responsible (see Infographic).  Not all patients who take the "triple whammy" combination develop kidney problems. To better understand the mechanism responsible for injury, researchers used computational models to gauge interactions. Their simulations suggested that low water intake, the myogenic response, and drug sensitivity may predispose certain patients to develop triple whammy–induced acute kidney injury. Without these additional risk factors, the risk was not elevated when an ACE inhibitor and NSAID were combined. In contrast, when an ACE inhibitor, diuretic, and NSAID are combined, critical BP and estimated glomerular filtration rate (eGFR) regulatory mechanisms are simultaneously interrupted. The "triple whammy" isn't the only drug combination that creates kidney concerns. A preprint study that has not yet been peer-reviewed examined which colorectal cancer regimens are most likely to result in acute kidney injury. The most likely culprit was FOLFIRI + bevacizumab. Prognostic factors included older age, low body mass index, and proteinuria at baseline. Across the four included regimens, patients' median eGFR fell from 90.9 mL/min/1.73 m2 at baseline to 80.1 mL/min/1.73 m2 at 12 months. Median 12-month eGFR among the 97 patients receiving FOLFIRI + bevacizumab fell the most, to 74.9 mL/min/1.73 m2. Incidence of acute kidney disease was lowest among patients treated with FOLFOX + cetuximab (2.1%) and highest among those who received FOLFIRI + bevacizumab (19.2%). In more encouraging kidney news, a recent study found that risks are low for donors. According to what is believed to be the largest study to date to examine the risks associated with living kidney donation via hand-assisted laparoscopic nephrectomy, the overall rate of complications was lower than that reported in some larger databases. Among 3002 living kidney donor nephrectomies, the overall complication rate was 12.4% (n = 371). Most were an infection or hernia related to the incision. The incidence of major complications was 2.5% (n = 74). Of these, 15 were intraoperative, 12 were postoperative to discharge, and 47 occurred after discharge to day 120 (all were reoperations, of which 46 were related to incisional issues). Not all kidney treatment-related news is as positive. A qualitative study recently found that Black veterans who have chronic kidney disease (CKD) report emotional and physical stress caused by racism in the medical setting. Researchers interviewed 36 Black veterans with CKD who were receiving care at the Corporal Michael J. Crescenz Veterans Affairs Medical Center. The mean age of participants was 66 years, and men comprised 97% of the study group. The qualitative data showed that Black veterans experienced physiologic symptoms (eg, headaches) and psychological symptoms of hurt and anger. They also felt a need to be hypervigilant during medical visits, which may be indicative of posttraumatic stress disorder. Outside of medical facilities, certain interventions may be beneficial in slowing kidney function decline. According to an analysis of randomized clinical trials, a structured moderate-intensity physical activity and strength/flexibility program in older adults (mean age, about 79 years) benefited kidneys. The program resulted in a statistically significantly lower decline in eGFR rate per cystatin C (eGFRCysC) compared with health education alone (mean difference, 0.96 mL/min/1.73 m2) and lower odds of rapid eGFRCysC decline (odds ratio, 0.79). Patients in the intervention arm underwent a structured, 2-year, partially supervised, moderate-intensity physical activity and exercise (strength and flexibility). Those in the health-education control arm attended weekly workshops. Cite this: Ryan Syrek. Trending Clinical Topic: Kidneys - Medscape - May 27, 2022.
By Susan Buckles Mayo Clinic Vulnerability to heart disease can be projected before symptoms occur, Mayo Clinic discovered in preclinical research. This proof-of-concept study revealed that heart muscle changes indicate who is vulnerable to disease later in life. These changes can be detected from blood samples through comprehensive protein and metabolite profiling. This exploratory mapping, conducted in the Marriott Family Comprehensive Cardiac Regenerative Program within Mayo Clinic's Center for Regenerative Medicine, is published in Scientific Reports.  "The team implemented state-of-the-art technologies to predict who is vulnerable and who is protected from heart disease," says Andre Terzic, M.D., Ph.D., a Mayo Clinic cardiologist and the senior author. "In this era of post-genomic medicine, the acquired foundational knowledge provides guidance for development of curative solutions targeted to correct the disease-causing maladaptation." Dr. Terzic is the Marriott Family Director, Comprehensive Cardiac Regenerative Medicine, for the Center for Regenerative Medicine and the Marriott Family Professor of Cardiovascular Research. Heart disease is a leading killer in the U.S., responsible for 1 of every 4 deaths, according to the Centers for Disease Control and Prevention. Predicting and intervening early in heart disease are health care priorities aimed at improving survival and quality of life while reducing health care costs. To address unmet needs of patients with chronic conditions such as heart disease, Mayo Clinic has invested in regenerative medicine and individualized medicine, transformative emerging fields in modern health care. Regenerative medicine seeks to restore the form and function of a failing or diseased organ, with individualized medicine tailoring care to a person's makeup. Mayo Clinic's Center for Regenerative Medicine is prioritizing clinical-grade biotherapeutics, targeting diseases with no cure. The research D. Kent Arrell, Ph.D. D. Kent Arrell, Ph.D. The research team mapped the molecular composition of hearts and discovered that in young adults, despite absence of any overt cardiac malfunction, deficiency in KATP channels -- innate safeguards of cardiac cell well-being under stress load — triggered heart tissue alterations that predict increased disease susceptibility. "We found that KATP channel deficit reorganizes the molecular identity of the heart. Notably, salient changes were also evident in blood, suggesting that heart vulnerability may be detected with a blood test, avoiding the need for invasive tissue biopsy," says D. Kent Arrell, Ph.D., first author. "Blood biomarkers could inform targeted biotherapeutic interventions for individuals deficient in natural cardiac protective capability." The team took a multiomics, high-tech systems approach to map the multiplicity of molecular changes. Going beyond the genome, thousands of distinct proteins and metabolites were deciphered, drawing a molecular atlas of cardioprotective deficiency.  Satsuki Yamada, M.D., Ph.D. Satsuki Yamada, M.D., Ph.D. "This proactive approach prior to disease onset offers an opportunity to maximize the success of future biotherapies aimed at addressing life-threatening conditions by correcting pinpointed deficits early in life that can be tailored for each individual," says Satsuki Yamada, M.D., Ph.D., a cardiologist and member of the study team.
Future clinical studies will be needed to translate these findings and ultimately advance diagnostics capable of predicting the risk of heart disease. Spending more time doing light-intensity activities and less time being sedentary was associated with a reduced risk for first stroke in a population-based study of middle aged and older adults. The study also found relatively short periods of moderate-to-vigorous exercise were associated with reduced stroke risk. "Our results suggest there are a number of ways to reduce stroke risk simply by moving about,” lead author Steven P. Hooker, PhD, San Diego State University, commented to theheart.org | Medscape Cardiology. "This could be with short periods of moderate-to-vigorous activity each day, longer periods of light activity, or just sedentary for shorter periods of time. All these things can make a difference." Hooker explained that it while it has been found previously that moderate-to-vigorous exercise reduces stroke risk, this study gives more information on light-intensity activities and sedentary behavior and the risk of stroke. "Our results suggest that you don't have to be a chronic exerciser to reduce stroke risk. Replacing sedentary time with light-intensity activity will be beneficial. Just go for a short walk, get up from your desk and move around the house at regular intervals. That can help to reduce stroke risk," Hooker said. "Our message is basically to sit less and move more," he added. The study is published online today in JAMA Network Open. The study involved 7607 US individuals without a history of stroke, with oversampling from the southeastern "Stroke Belt," who were participating in the REGARDS cohort study. The participants wore an accelerometer to measure physical activity and sedentary behavior for seven consecutive days. The mean age of the individuals was 63 years; 54% were female, 32% were Black. Over a mean follow up of 7.4 years, 286 incident stroke cases occurred. Results showed that increased levels of physical activity were associated reduced risk of stroke. For moderate-to-vigorous activity, compared with participants in the lowest tertile, those in the highest tertile of total daily time in moderate to vigorous activity had a 43% lower risk of stroke. In the current study, the amount of moderate-to-vigorous activity associated with a significant reduction in stroke risk was approximately 25 minutes per day (3 hours per week). Hooker noted that moderate-to-vigorous activity included things such as brisk walking, jogging, bike riding, swimming, playing tennis or soccer. "Doing such activities for just 25 minutes per day reduced risk of stroke by 43%. This is very doable. Just commuting to work by bicycle would cover you here," he said. In terms of light-intensity activity, individuals who did 4-5 hours of light activities each day had a 26% reduced risk for first stroke compared with those doing less than 3 hours of such light activities. Hooker explained that examples of light activity included household chores, such as vacuuming, washing dishes, or going for a gentle stroll. "These activities do not require heaving breathing, increased heart rate or breaking into a sweat. They are activities of daily living and relatively easy to engage in." But he pointed out that the 4-5 hours of light activity every day linked to a reduction in stroke risk may be more difficult to achieve than the 25 minutes of moderate-to-vigorous activity, saying: "You have to have some intentionality here." Long Bouts of Sedentary Time Are Harmful The study also showed that sedentary time was associated with a higher risk for stroke. The authors note that time spent in sedentary behavior is of interest because most adults spend most of their awake time being physically inactive. They report that participants in the highest tertile of sedentary time (more than 13 hours/day) exhibited a 44% increase in risk of stroke compared with those in the lowest tertile (less than 11 hours/day), and the association remained significant when adjusted for several covariates, including moderate to vigorous activity. "Even when controlling for the amount of other physical activity, sedentary behavior is still highly associated with risk of stroke. So even if you are active, long bouts of sedentary behaviour are harmful," Hooker commented. They also found that longer bouts of sedentary time (more than 17 minutes at a time) were associated with a 54% higher risk of stroke than shorter bouts (less than 8 minutes). "This suggests that breaking up periods of sedentary behavior into shorter bouts would be beneficial," Hooker said. "If you are going to spend the evening on the couch watching television, try to stand up and walk around every few minutes. Same for if you are sitting at a computer all day — try having a standing workstation, or at least take regular breaks to walk around," he added.
This research was supported by grants from the National Institute of Neurological Disorders and Stroke (NINDS) and the National Institute on Aging (NIA). Additional funding was provided by an unrestricted grant from the Coca-Cola Company. The authors report no disclosures. JAMA Netw Open. Published online June 3, 2022. Credits to MEDSCAPE Article
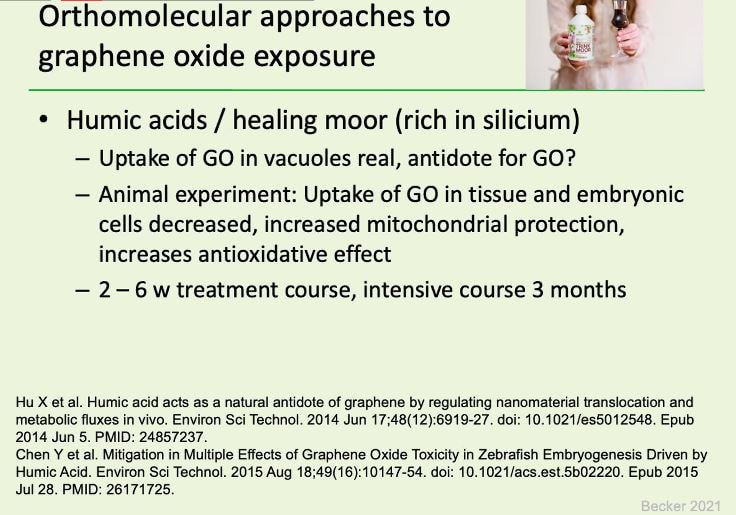
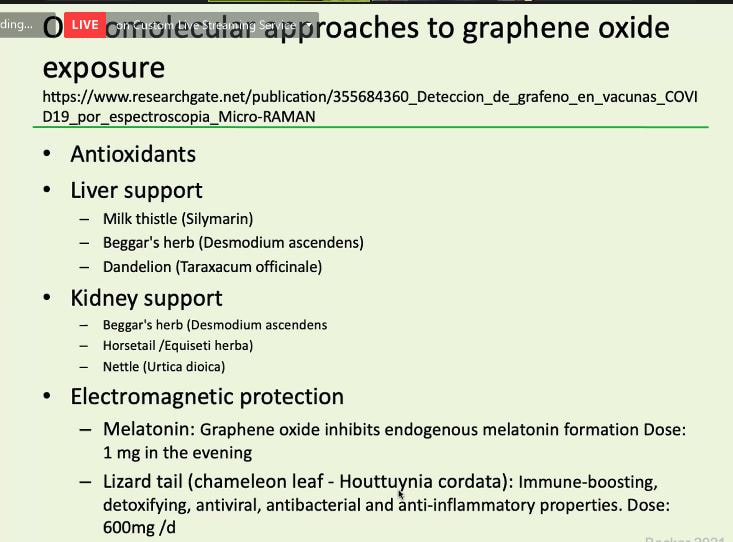
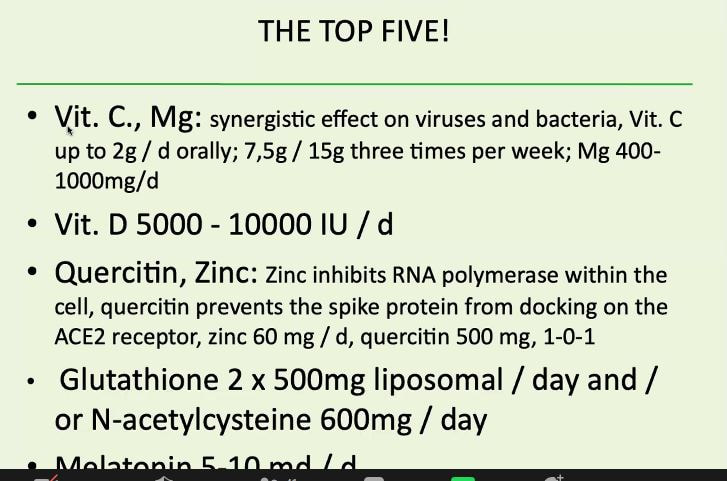
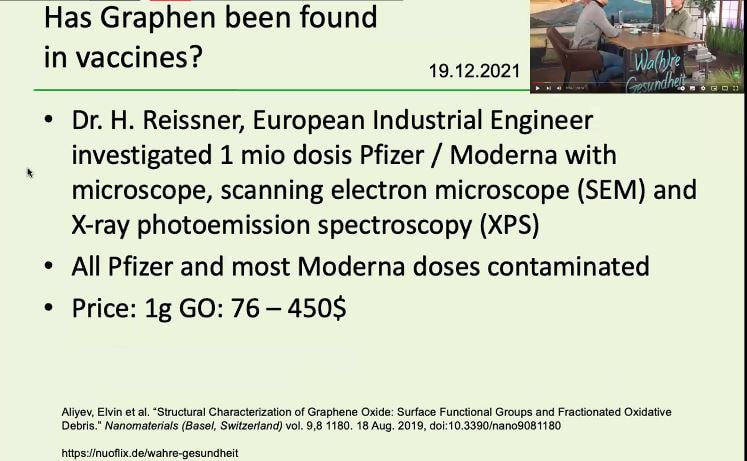
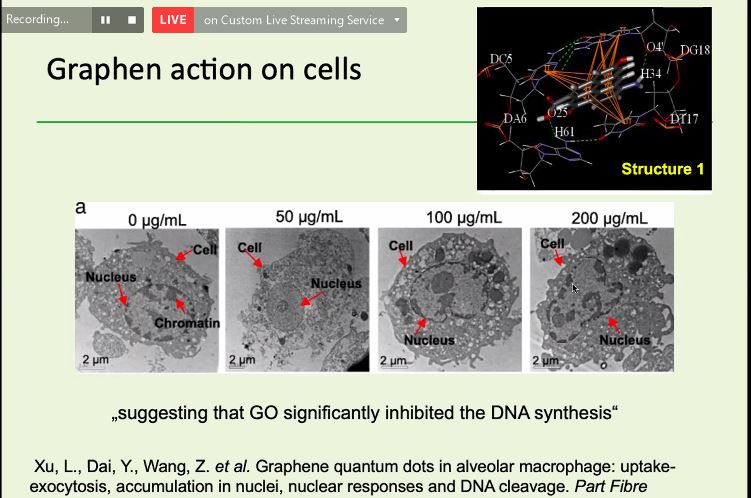
Dr. Stephan Becker on the Jab induced Injuries Management
Dr. Stephan Becker, a specialist in orthopedic surgery, has already gained a lot of international experience and has also dealt intensively with immunology. This is the recent roundtable discussion among physicians all over the globe discussing/reporting/sharing treatment regimens/studies and experience in the treatment and management of the current pandemic malady. The event was hosted by Dr. Nasseba Kathrada and co-hosted by yours truly. At present, I am not doing any of my original content as we are loaded with virtual meetings and round table discussions. What I am doing now, as a steering committee member of WCH or World Council for health is to also share content on what has been discussed on Round table discussions, health summits, and general assembly meetings.
Dr. Tess Lawrie: An insight into the conversation between Dr. Tess Lawrie & Dr. Andrew Hill, as published in Robert F. Kennedy’s book The Real Anthony Fauci
Dr. Tess Lawrie (MBBCh, PhD) is the Director of the Evidence-based Medicine Consultancy Ltd, and CEO of EbMCsquared CiC, an independent, not for profit, health-focused think tank based in the United Kingdom. She is also the founder of the British Ivermectin Recommendation Development initiative (now called BiRD International) and a co-founder of World Council for Health. |

AUTHOR
An approach to healing that considers the whole person -- body, mind, spirit, and emotions -- in the quest for optimal health and wellness. Most of the time I share articles from different journals with atributions and sometimes I write articles. Blockchain based
Medical Certificate

The OPHIR Cryptocurrency is a decentralized endowment token designed for unlocking abundance to fuel generosity; empowering & resourcing grassroots churches and those advocating for the poor and vulnerable across the Philippines and the world.
LISTEN TO SOOTHING LOFI FOCUS MUSIC. Play BELOW

Blockchain based Birth Registry
Boost your immune system with intra

Archives
April 2023

Streamyarrd your Livestreaming Solutions

TAMANU OIL by XQUISSENTIALS
ANTI-AGING, CELLULAR REJUVINATING OIL

It's convenient Load your phone, pay bills, and receive money from anyoneTake extra time with your morning coffee, and skip the lines. We'll do the rest for you. Coins.ph is on a mission to make your everyday life simpler, more pleasant, and more rewarding.

|




 RSS Feed
RSS Feed
